

Cardiovascular disease remains the leading cause of death in the United States and worldwide. The National Institutes of Health’s National Library of Medicine observes that congestive heart failure (HF) has been described as the new epidemic, and despite advances in drug therapy, a two-year mortality of up to 50 percent persists.
In the U.S. alone, about 5 million people suffer from HF and almost one million are hospitalized annually. The annual cost to the U.S. healthcare system is estimated at over $40 billion, and the number of patients diagnosed with HF is expected to double within the next decade as baby boomers age.
There are limitations to current drug treatments and cardiac resynchronization devices; furthermore, the treatment of diastolic dysfunction can be suboptimal. HF is a costly, challenging and highly prevalent medical condition, and a major public health concern given the associated acute decompensated HF (ADHF), a sentinel event signifying disease progression and the inability of the heart to maintain adequate hemodynamics for the perfusion and function of vital organs.
According to a new Open Access study published in the journal Frontiers in Physiology, nearly half of the HF patients are readmitted to hospitals within six months and/or die within a year. The lifetime risk of developing HF for Americans aged 40 years or older is approximately 20 percent, with the incidence of new HF cases now exceeding 650,000 annually.
The paper entitled “Evolution from electrophysiologic to hemodynamic monitoring: the story of left atrial and pulmonary artery pressure monitors” (Front Physiol. 2015; 6: 271. Published online 2015 Oct 7. doi: 10.3389/fphys.2015.00271 PMCID: PMC4595778), is co-authored by Deirdre M. Mooney of the Maine Medical Center Cardiovascular Institute in Portland, Maine, and Tufts University School of Medicine in Boston, Massachusetts; Rahul N. Doshi and David M. Shavelle of Keck Medical Center of USC, University of Southern California, Los Angeles; and Erik Fung, also associated with Keck Medical Center as well as the Department of Medicine at Dartmouth College in Hanover, New Hampshire, and the School of Public Health at Imperial College London, U.K. The research team notes that over one million hospitalizations are attributed to HF annually and emphasize that hospitalization for ADHF is associated with high morbidity and mortality, and can impose major financial stress on institutions and resources.
Accordingly, to contain costs and standardize management of patients hospitalized for ADHF, the co-authors report that the Centers for Medicare and Medicaid Services have recently introduced regulations to withhold or reduce payments for unnecessary hospitalizations for HF. Increasingly coming under closer scrutiny are readmission rates and other performance metrics (e.g., length of hospital stay, medical regimen at discharge) that are fueling efforts to reduce HF readmission.
Evidence-based therapies, including optimal medical therapy with neurohormonal antagonists and implantable devices (e.g., cardiac resynchronization therapy, defibrillators), are well-outlined by major cardiovascular and electrophysiological societies, including the American College of Cardiology, American Heart Association, Heart Failure Society of America, European Society of Cardiology, European Heart Rhythm Association, and Heart Rhythm Society. Nonetheless, despite application of these treatments and technologies, HF remains a formidable challenge for virtually all healthcare systems. Moreover, the quality of evidence for care, support and monitoring systems, as well as the infrastructure to support HF patients, particularly in the outpatient setting, is lacking.
Consequently, the team observed that early and accurate identification of impending ADHF is of paramount importance, yet high quality evidence or infrastructure to guide management in outpatient settings is limited. It notes that, historically, ADHF was identified by physical exam findings or invasive hemodynamic monitoring during a hospital admission.
However, the investigators report that advances in medical microelectronics and the advent of device-based diagnostics have enabled long-term ambulatory monitoring of HF patients in the outpatient setting. These monitors have evolved from piggybacking on cardiac implantable electrophysiologic devices to standalone implantable hemodynamic monitors that transduce left atrial or pulmonary artery pressures as surrogate measures of left ventricular filling pressure.
The co-authors maintain that as the technology evolves, these devices will likely continue to miniaturize while their capabilities expand. But they note that an important and persistent challenge is the development of systems to translate large volumes of real-time data — particularly data trends — into actionable information that leads to appropriate, safe, and timely interventions without overwhelming outpatient cardiology and general medical practices. They suggest that future directions for implantable hemodynamic monitors will expand beyond their utility in heart failure and may include management of other major chronic diseases, such as pulmonary hypertension, end-stage renal disease and portal hypertension.
For example, they point to the recent development and clinical trials of implantable hemodynamic monitoring devices as holding promise for reducing HF hospitalizations, as well as the potential to improve patient outcomes. They also underscore the importance of careful clinical trial design, endpoint selection, outcome assessment, management of actionable results, and other ethical issues.
The Frontiers in Physiology paper focuses on implantable hemodynamic monitors that evolved from electrophysiologic (EP) devices with extended functionality to dedicated standalone pulmonary artery pressure monitors for guiding medical management of hemodynamic and volume status in outpatients, with demonstrable effects on reducing hospital readmission.
Noting that early and accurate identification of impending and active ADHF is of paramount importance, the investigators point to daily weight monitoring as a low-cost, easily accessible method of monitoring HF patients both in and out of the hospital. Unfortunately, however, weight as a reference value is easily confounded by changes in diet and muscle mass that are not related to intravascular volume status or filling pressures, and the researchers cite previous studies that found the estimated positive predictive value for these findings to be generally poor. Moreover, while tele monitoring and collaborative multidisciplinary outpatient care teams appear to be practical and effective measures to improve HF management, randomized studies have yet to confirm this, and the clinical symptoms of dyspnea, orthopnea, weight gain, and leg edema are often late indicators of congestion and volume overload that may already warrant hospitalization.
Physical examination maneuvers such as inspection of the jugular venous pressure waveform, hepatojugular reflux and the square wave sign are useful surrogate measures of cardiac filling pressures, although inter- and intra-observer variability, inconsistent manifestations, and the need for the patient to present for a physical examination limit their applicability to identify early decompensated heart failure in the outpatient setting. Additionally, the sensitivity and specificity of these signs and symptoms vary widely, depending on the clinical study.
The co-authors report that a gold standard measure of congestion in HF is not overall volume status, but rather the pulmonary artery occlusion pressure, also known as the pulmonary capillary wedge pressure (PCWP), which reflects left-sided cardiac filling pressures and is measured by a pressure transducer on the end of a pulmonary artery catheter. An inflatable balloon allows placement of the catheter into a sub-selected pulmonary artery (PA) branch. An elevated PCWP, exceeding 18–22 mm Hg, indicates pulmonary edema and congestion. Given the potential dangers of an indwelling PA catheter for invasive hemodynamic monitoring, the patient is by convention required to stay in the intensive care unit.
The paper points to advances in medical microelectronics and the advent of device-based diagnostics that have been developed to enable monitoring of ambulatory HF patients, with the ability to transmit and report objective, quantitative data via remote monitoring systems. The premise of monitoring physiologic parameters, they observe, is to enable clinicians to use these surrogate markers to optimize the patients’ medical therapy in the ambulatory setting.
Several of the currently available tele monitoring systems measure various cardiac pressures, and tailoring of medical therapy based upon these pressures, known as pressure guided therapy, is based on the observation that most patients with HF require hospitalization because of excessive fluid accumulation. Because fluid accumulation occurs over several weeks, timely knowledge of these pressure increases can allow adjustment of medications to avoid reaching this threshold and a hospital stay.
An effective HF monitor would be a programmable device resembling a pacemaker pulse generator, implanted to process and store information from the pressure sensor near the tip of the transvenous lead. The device continuously records data, such as heart rate, body temperature, estimated patient activity level, right ventricular (RV) systolic and diastolic pressure, RV pressure changes, and estimated PA diastolic pressure. In the COMPASS-HF trial, patients were asked to use a handheld radio frequency device to transmit readings at least once weekly using a telephone line. Information was stored on a server that clinicians could access through a secure website.
The Savacor Company, which was acquired in 2005 by St. Jude Medical of St. Paul, Minnesota — a biotech firm pioneering HF disease management with innovative solutions that help reduce hospitalizations and improve the quality of life of patients — developed the HeartPOD device to directly measure left atrial pressure in patients with congestive heart failure via an implantable device. The HeartPOD device consists of a permanently implanted intracardiac microelectronic sensor and diaphragm housed in a cylindrical titanium casing (approximately 3 mm by 7 mm) equipped with deployment anchors, and linked with an implantable sensor lead and a coil antenna that allows the patient to directly monitor left atrial pressure, the intracardiac electrogram, and core body temperature. The device is implanted by a minimally invasive cardiac catheterization procedure, similar to pacemaker insertion. The implant’s readings are communicated with a hand-held computer called a Patient Advisory Module, or PAM. The information is used to adjust medications on a dose-by-dose basis according to the patient’s physician’s prescriptive instructions. This permits real-time adjustment and dosing of medication similar to the way diabetics adjust insulin dosage in response to home glucose monitoring. Left atrial pressure is believed to be a key measurement for predicting acute worsening of HF that leads to lung congestion and the need for urgent hospitalization.
The CardioMEMS HF System (St. Jude Medical Inc., Sylmar, California, office) is the first and only FDA-approved HF standalone monitoring system proven to significantly reduce HF hospital admissions and improve quality of life in patients. The CardioMEMS device was developed to directly measure systolic, diastolic and mean PAPs using a miniaturized wireless electromechanical sensor implanted in conjunction with a right heart catheterization procedure via transvenous access.
CardioMEMS was tested and proven to significantly reduce patient admissions (New York Heart Association functional class III HF patients), regardless of left ventricular ejection fraction (LVEF), even in those with HF with preserved LVEF as opposed to those with reduced LVEF. A large post-approval trial is already recruiting (goal N=1200) to verify the robustness, safety and usefulness of CardioMEMS in the complex real-world setting, particularly in reducing the rate of HF hospital readmissions and in improving patients’ quality of life.
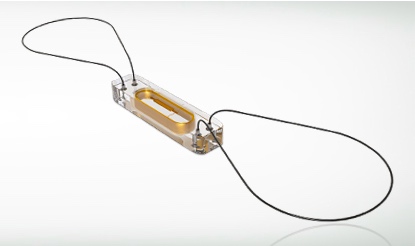
CardioMEMS is a battery-free, leadless sensor (15 mm by 3 mm) consisting of a coil and capacitor encased in silicone, with a nitinol wire loop at each end of the sensor. The device is preloaded on a delivery catheter with a tether release system. The design of the system is based on microelectromechanical principles of resonance, whereby an external antenna wand emitting radio frequency energy can cause varying degrees of oscillations in the sensor depending on the ambient pressure.

Both the HeartPOD and CardioMEMS systems use a physician-guided, intuitive, and conceptually sound self-management model. The study co-authors cite experts in the field who have universally acknowledged the challenges in conducting implantable monitoring trials to demonstrate impacts on clinical outcomes, particularly with how the interrogated physiologic data are handled. Successful monitoring of device data requires both patient and physician compliance, and a structured action plan or algorithm to execute it.
 According to William Abraham, MD, FACC, Chief of Cardiology at Ohio State University, Columbus, Ohio: “Left atrial pressure is the measurement we’ve been waiting for because when it is too high, it is the proximate cause of water accumulating in the lungs, which is responsible for 90 percent of HF hospitalizations, and when it is too low, damage to the kidneys may occur, which carries a three- to four-fold increase in mortality.”
According to William Abraham, MD, FACC, Chief of Cardiology at Ohio State University, Columbus, Ohio: “Left atrial pressure is the measurement we’ve been waiting for because when it is too high, it is the proximate cause of water accumulating in the lungs, which is responsible for 90 percent of HF hospitalizations, and when it is too low, damage to the kidneys may occur, which carries a three- to four-fold increase in mortality.”
It is suggested that achieving the goal of reducing patient hospitalization and readmission for HF requires a team effort involving the patient, caretaker, primary care physician, cardiologist, nurse and/or support staff. Such a team will require sufficient resources and training to appropriately interpret data trends, and standard easy to use protocols would lead to more uniform management and optimize the ability to study implantable hemodynamic monitor devices. The researchers say these protocols will need to have some flexibility so healthcare providers can customize treatment plans to each individual.
The co-authors note that in monitoring data, it has been emphasized that data trends are more crucial to successful management than acting on individual abnormal data points, and potential harm could also be introduced with injudicious remote monitoring when treatments, such as diuretic therapy and vasodilators, are administered without careful consideration, understanding, and interpretation of abnormal data. Establishing a good line of communication with the patient and exercising clinical judgment (e.g., focused history taking to gather clinical cues, scheduling an outpatient visit when required, and assessing renal function and/or electrolytes after adjustment of medical therapy such as diuretics), may help to clarify abnormal and outlying data trends.
An online secure website (https://cardiomemshf.com/user/sign_in) is accessible to healthcare professionals to view the interrogated data. The HeartPOD, CardioMEMS and other non-EP (i.e., without pacemaking or defibrillator functions) implantable monitoring systems have built-in, untapped features including cardiac output, heart rate variability, and electrocardiographic monitoring.
In summary, the researchers concluded that with implantable cardiovascular devices, a wealth of data can be harnessed through minimally invasive means and transmitted to a secure data repository via remote wireless technology. Newer implantable cardiac monitoring devices for HF offer the ability to provide individualized data trends and ideally predict clinical events before they occur. However, isolated device alerts need to be used in conjunction with other clinical data to avoid over-utilization of healthcare resources and an increase in hospitalizations. Successful translation of remote device-based monitoring into successful clinical management of patients will require simple prospectively validated algorithms that indicate how to use raw data from individual devices to make timely and appropriate changes in clinical management without overburdening staff. At this time, despite a wealth of smaller studies evaluating these devices, the co-authors say larger clinical randomized trials are necessary to demonstrate that implantable device-based hemodynamic sensors beneficially impact morbidity and mortality in HF patients.
Sources:
Frontiers in Physiology
National Institutes of Health’s US National Library of Medicine
St. Jude Medical Inc.
